

 Jenee Virtudazo , RND, MPH
Jenee Virtudazo , RND, MPH
Introduction
Diabetes mellitus, a group of diseases characterized by high blood sugar or hyperglycemia – the result of defects in insulin secretion, insulin action or both – is a serious health issue. In fact, the Philippines ranked 15th in the world for diabetes prevalence, making the country home to more than 4 million individuals diagnosed with the disease.1 The data below shows the prevalence of diabetes mellitus in the Philippines for the last 10 years according to the National Nutrition and Health Survey:
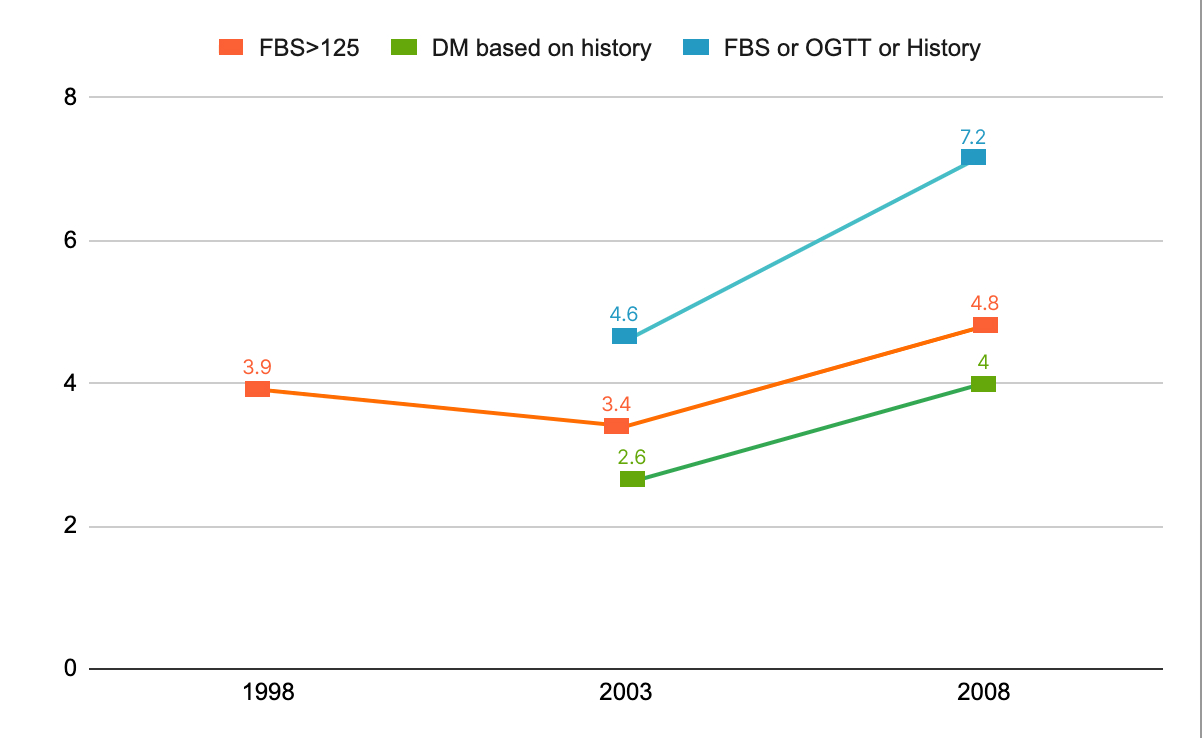
Figure 1. Prevalence of Diabetes Mellitus in the Philippines from 1998-20082
In 1998, the prevalence of DM based on a fasting blood glucose of greater than 125 (mg/dl) is 3.9%. In 2003, the prevalence increased to 10.6% using the classification of having FBS > 125 mg/dl, history of DM and a combination of FBS, oral glucose tolerance test (OGTT) or history. In 2008, the prevalence of DM grew to 16%. The above figure balloons to 17.8% or 20% after adding those who have pre-diabetes (FBS > 99 mg/dl) impaired fasting glucose or impaired glucose tolerance or both) which has prevalence of 10.6%. This means that 1 out of every 5 Filipinos could potentially have diabetes mellitus or pre-diabetes. The research conducted by the Philippine Diabetes Care in 2008 furthermore showed that 85% of patients with DM failed to achieve a general HbA1c target of <7%.
The latest research conducted regarding Philippine diabetes care was in 2008 which showed that 85 percent of patients with diabetes failed to achieve a general HbA1c target of <7 percent. Diabetes mellitus ranks 4th in the All Cause Mortality data of the Philippine Statistics Authority (Figure 1).
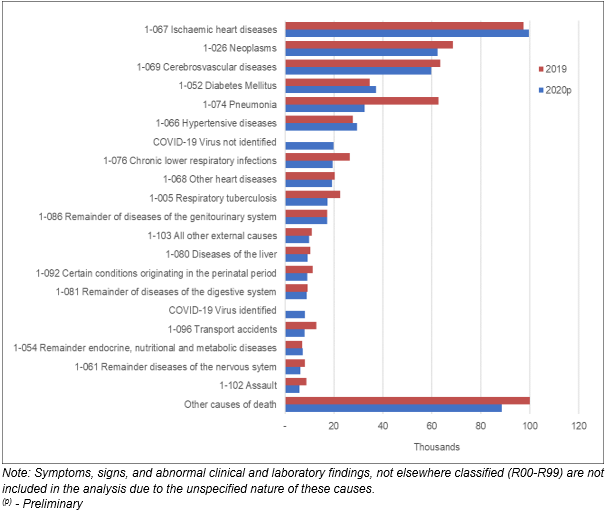
Figure 2. All Cause Mortality (Top 20), Philippines: January to December, 2019 & 20203
Manage your sugar, manage your diabetes
Managing blood sugar levels and carbohydrate intake is essential in keeping a healthy body whether you’ve been diagnosed with diabetes or not. Good blood sugar (glycemic) control is proven to decrease microvascular disease complications and provides long-term prevention of heart or cardiovascular disease. There is compelling evidence that improved glycemic control reduces risks of development and/ or progression of microvascular complications in type 2 diabetes.
The primary prevention of diabetes complications is good glycemic control. What are the targets for glycemic control? Glycemic targets must be individualized. One common test is A1C or HbA1c test, a simple blood test that measures blood glucose levels over the past three months.
A target of A1C of <7.0% should be considered in all patients with type 2 diabetes in order to reduce microvascular complications.
In order to achieve A1C of 7.0%, people with diabetes should aim for2:
- A preprandial or before meal plasma glucose (PG) target of 4.0 to 7.0 mmol/L (72 to 126 mg/dl). [Grade B, Level 21, for type 1; Grade B, Level 22,3, for type 2 diabetes]; and
- A 2-hour postprandial or after meal PG target of 5.0 to 10.0 mmol/L (90 to 180 mg/dL) [Grade B, Level 21, for type 1 diabetes; Grade B, Level 22,3, for type 2 diabetes].
- Alternatively, capillary blood glucose targets can be: FBS 90-130 mg/dL (ADA), PPBG <180 (ADA).
A target of <6.5% may be optimal for certain types of patients such as those with short duration of diabetes, long life expectancy, no significant active cardiovascular disease, no serious comorbid risk factors and at those with low risk for cardiovascular events that may be triggered by hypoglycemia.
In order to achieve a target of A1c <6.5%, the patient must achieve the following plasma glucose level2:
- Preprandial (before meal): <6.0 mmol/L (or <110 mg/dl)
- Postprandial (after meal): <8.0 mmol/L (or <145 mg/dl)
When left untreated, complications of diabetes in the small blood vessels range from retinopathy (disease of the eyes that may lead to blindness), nephropathy (kidney disease) and neuropathy (nerve problems). Common consequences of diabetic neuropathy and/or arterial disease, include foot ulcers and amputations, and/or sickness and death.
To achieve glycemic control, it warrants a well-focused and individualized nutrition therapy. We have either heard or read several recommendations on what to eat or what not to eat to help achieve near normal blood glucose levels. So much controversy and questions arise with regards to diabetes and food intake. Same way that there are popular myths and facts pertaining dietary intake and diabetes. The following are some of the myths and an explanation of the facts about it.
Myth No. 1. “Soda is a sugary drink. Therefore, it should be avoided to prevent or manage diabetes. Fruit juice is allowed as long as it is unsweetened.”
Fact:
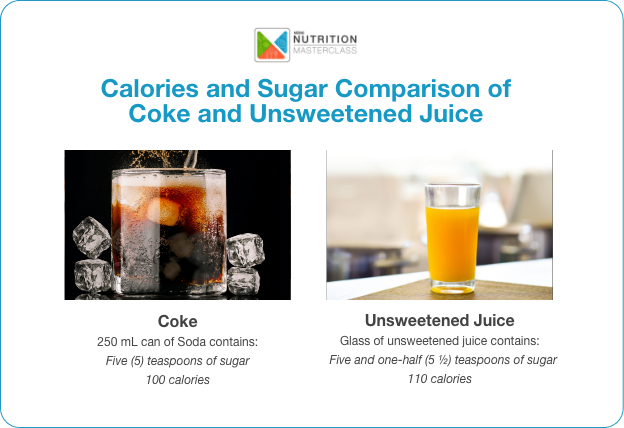
A 250 mL can of soda contains five (5) teaspoons of sugar and around 100 calories. A glass of unsweetened orange juice, on the other hand, despite having fructose, a type of sugar that occurs naturally in fruits, contains an equivalent of five and one-half (5 ½) teaspoons of sugar and 110 calories of energy.4
Both soda and unsweetened fruit juice contain a considerable amount of sugar per can or per 250 mL measure. In this example, one can of unsweetened orange juice actually has higher calories and sugar content than that of a 250 mL soda.
Unsweetened fruit juices do not always mean sugar free. The natural sugar content of fruits called fructose is easily converted to glucose (blood sugar) and thereby can also lead to high blood sugar.
Myth No. 2: “I consume less calories by avoiding rice and eating bread instead. This way, I avoid getting high blood sugar.”
Fact:
One half cup of rice (80g) has 100 calories, 23g of carbohydrates, and 2g protein. Two slices of Pan Americano or loaf bread (35g) contains 108 calories, 23g carbohydrates, and 4g protein.4
Each gram of rice has:
| Each gram of bread has:
|
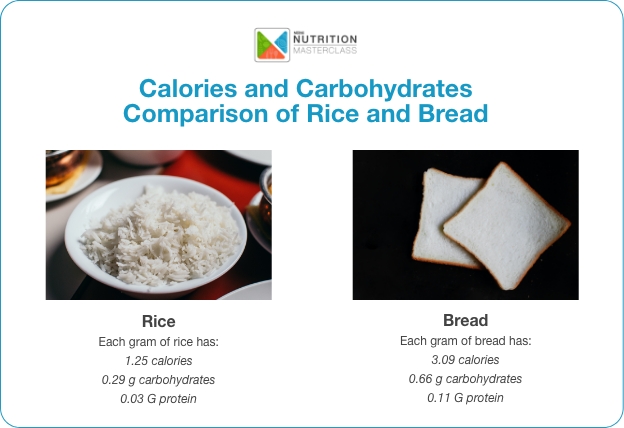
Carbohydrates should not be totally avoided but instead be made a part of a healthy, balanced diet. They should be a staple in every meal with specifications on the amount recommended for meals and snacks, if so desired. Together with proteins and fats, it should be eaten as consistently as possible for a balanced meal plan.
Myth No. 3: “I only drink coffee in the morning, so I can eat more during lunch.”
Facts:
Keeping a proper schedule for meals is just as important as the amount and type of food you eat. Taking very small amounts of food during breakfast increases the risk of hypoglycemia or low blood sugar. Eating more food at a certain mealtime, on the other hand, may lead to hyperglycemia or high blood sugar. Having blood sugar that is too low or too high can lead to complications.
Skipping meals is not the way to go as doing so can also lead to overeating later in the day, which can cause blood sugar spikes. People who are not eating balanced meals are susceptible to night time hypoglycemia or nocturnal hypoglycemia. This is dangerous mainly because you do not feel the symptoms of hypoglycemia. Eating a balanced breakfast, lunch and dinner with in-between snacks can help achieve near normal blood sugar levels.
Misconceptions such as skipping meals and completely avoiding rice, sugar or fruit should be corrected. Here are some of the simple reminders of the Asia-Pacific Type 2 Diabetes Policy Group2:

Myth No. 4: “I have no risk of developing diabetes later in life because it doesn’t run in the family.”
Fact:
Diabetes can develop at any age and there are other risk factors aside from family history. The chances of developing diabetes depends on a combination of the following risk factors5:
- If you are overweight or obese
- If you are aged 35 or older
- If you are not physically active
- If you have prediabetes (100-125 mg/dL)
- If you have history of gestational diabetes
- If you have history of diabetes in the family
- If you are African American, American Indian, Asian American, Hispanic/Latino, or Pacific Islander
Myth No. 5: “I will not be able to enjoy delicious food because I have diabetes.”
Fact:
It is a misconception to think that having diabetes means not getting to enjoy the food you like and that there are too many restrictions regarding eating your favorite food. The truth is you can still enjoy your favorite food but in moderation – you will need to make the portions smaller and enjoy them less than often.
The key to eating with diabetes is to eat a variety of healthy foods from all food groups as outlined in the meal plan.
Using natural condiments and spices such as garlic, onion, tomatoes, red and green bell peppers, black and white pepper, curry and chili peppers will add extra flavor to the food without increasing sodium in the diet. Lessen the use of salty condiments like soy sauce and fish sauce most especially if a person has hypertension.
Myth No. 6: “My HbA1c blood test result came back normal, does this mean my diabetes is cured?”
Fact:
Once diagnosed a diabetic, always a diabetic. Sadly, there is no existing cure for diabetes at the moment. The good news however is that diabetes can be controlled to a point that when blood sugar is maintained to attain near normal levels, it is as if there is no diabetes at all. But once a patient forgets or fails to comply with the medical and nutrition recommendations, the symptoms and other manifestations of the disease will once again show.
Doable, Healthy Meal Plan for Patients with Diabetes
Unbeknownst to us, we do menu planning every day but we are unconscious that we are doing it. When you think of what to cook for breakfast, what to eat for lunch or what to prepare for dinner, even just deciding what to eat for each meal is menu planning. To be able to serve a healthy meal every time, it is important to ensure that there is a representative from the three food groups in every meal:
Go Food
Purpose: For energy-giving
Source: Carbohydrates and fat
Grow Food
Purpose: For building and repairing
Source: Protein-rich food
Glow Food
Purpose: For body regulating and gut health
Source: Vitamins, minerals and fiber

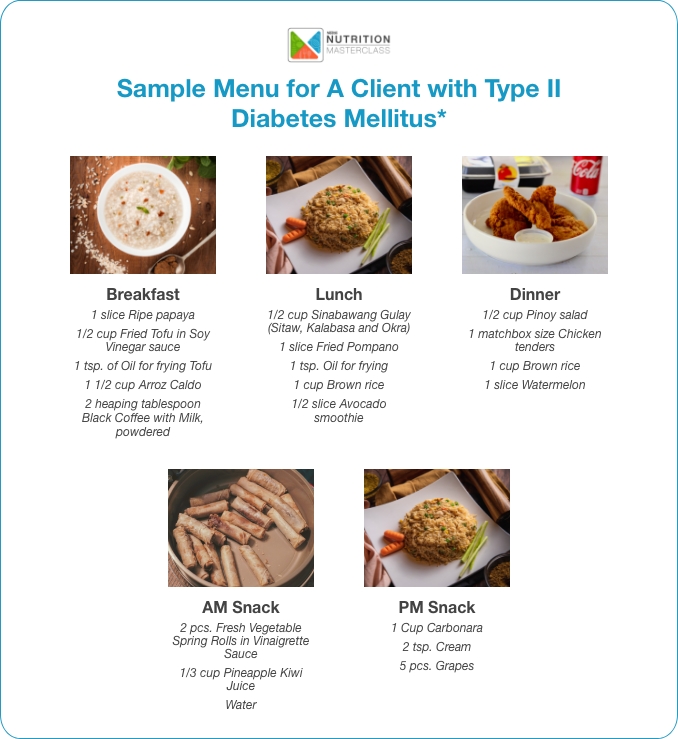
Sample Menu for A Client with Type II Diabetes Mellitus
Conclusion
It takes proactive measures to prevent diabetes from worsening or getting out of control. Don’t make the mistake of believing myths and misconceptions about diabetes, lest you will think living with diabetes is restrictive and unhappy. Simple adjustments such as reducing sugar and carbohydrates intake and managing a healthy eating schedule and plan are all essential to living a holistic life even with diabetes.
Message to RNDs
All individuals at risk for diabetes – those with pre-diabetes or diabetes and overweight individuals with metabolic syndrome – should be given advice to attain treatment targets. Managing blood glucose is one of the cornerstones of living well with diabetes mellitus. Healthy eating is the key to successfully attaining blood glucose at any stage of nutrition therapy.
The most valuable player (MVP) in the Medical Nutrition Therapy (MNT) for diabetes mellitus is a Registered Nutritionist Dietitian. The nutrition therapy of DM clients requires individualization and is very important for the secondary prevention of diabetes complications. The complications are inevitable but good or tight blood glucose control will prolong the appearance of complications. It is the RND’s role to explain the value of dietary compliance to delay the onset of the following complications, including nephropathy, retinopathy, neuropathy, coronary artery disease, disability due to non-healing wounds, and amputation.















No comments here yet.